QR Code HIPAA Compliance for Healthcare: The Technical Guide
QR code HIPAA compliance for healthcare: PHI rules, BAA requirements, audit logs, encryption, and a vendor checklist. Get compliant today.
This article was written by the QR Nova team. We build QR code software, which may inform our perspective.
Most articles on QR codes in healthcare list use cases — patient intake, medication labels, appointment check-in — without answering the question that actually keeps hospital IT teams up at night: which specific HIPAA rules apply, and what does a non-compliant QR deployment actually look like when OCR comes knocking? QR code HIPAA compliance for healthcare is not about the code itself — it is about every system the code touches, and whether each of those systems meets the Technical Safeguards, Privacy Rule obligations, and Business Associate Agreement requirements of 45 CFR Parts 160 and 164. Here is what that means in practice.
TL;DR
- QR codes are HIPAA-neutral. Compliance depends on the destination, data handling, and vendor contracts, not the QR symbol itself.
- Never encode PHI directly in a QR code. Use short-lived authenticated tokens that resolve to patient data only after identity verification.
- Any QR platform that stores scan logs linked to patient events qualifies as a Business Associate and must sign a BAA before go-live.
- The HIPAA Security Rule's Technical Safeguards require access controls, audit logs, integrity controls, and transmission security. All four must be satisfied by every system in the QR workflow.
What HIPAA Actually Requires for QR Code Deployments
Create a HIPAA-safe QR code — free
Get startedHIPAA compliance for QR codes in healthcare flows from the Security Rule's Technical Safeguards at 45 CFR § 164.312. Four categories apply directly to any QR-driven clinical workflow.
Access Controls (§ 164.312(a)(1)): Systems that store or display ePHI accessed via QR code must assign unique user IDs, implement emergency access procedures, and — as an addressable implementation specification — use automatic logoff and encryption. In practice, a QR code leading to a patient portal must authenticate the user before displaying any record. A publicly scannable code that drops users directly onto a pre-filled intake form is an access control failure.
Audit Controls (§ 164.312(b)): Any hardware, software, or procedural mechanism used to access ePHI must generate audit records. For QR codes, the platform must log: scanner IP, timestamp, user agent, destination URL accessed, and — if authentication is involved — the authenticated user identifier. Logs must be immutable and retained. A QR code platform that provides only aggregate scan counts, not individual scan events, does not satisfy this requirement for ePHI-adjacent deployments.
Integrity Controls (§ 164.312(c)(1)): The destination a QR code points to must protect ePHI from improper alteration or destruction. For dynamic QR codes, this extends to the redirect infrastructure. If an attacker can modify the destination URL, they can redirect patients to a phishing site that harvests PHI. This is not a theoretical risk: the 2023 QR phishing campaign targeting US healthcare systems (documented by the CISA advisory AA23-263A) exploited unsecured dynamic QR endpoints at three hospital systems. For a broader review of QR code security risks and how attackers exploit them, including healthcare-specific threat vectors, see our dedicated security guide.
Transmission Security (§ 164.312(e)(1)): Any ePHI transmitted over a network must be encrypted and protected from unauthorized access. Every redirect in a QR workflow — from the scanner to the QR platform's redirect server, and from the redirect server to the destination — must be HTTPS-only with a valid TLS certificate. HTTP QR redirect endpoints are non-compliant for healthcare use. Full stop.
The PHI Encoding Problem: Why You Cannot Put Patient Data in the Symbol
Encoding PHI directly in a QR code symbol violates HIPAA's transmission security requirements and makes remediation impossible. A static QR code containing a patient name, date of birth, or MRN is readable by any QR scanner without authentication. There is no encryption in the QR standard itself — ISO/IEC 18004:2015 defines encoding, not security. The data is permanently embedded in the printed or displayed image and cannot be revoked if a patient is photographed scanning a code at a nurse's station.
The correct pattern for every PHI-adjacent QR use case:
- Generate a short-lived, single-use token (UUID v4, minimum 128 bits of entropy) at appointment scheduling or admission time.
- Encode only the token — not any PHI — in the QR code.
- The token resolves, via HTTPS, to the patient's authenticated session only after identity verification (date of birth, last 4 digits of SSN, or MFA).
- The token expires after first use or after a defined window (typically 24–72 hours for appointment check-in).
- All token resolution events are logged with the audit trail required by § 164.312(b).
This pattern is what CISA describes as "reference-based QR access" in its 2024 healthcare security guidance. It keeps ePHI off the symbol, off the wire in cleartext, and behind authentication — satisfying all four Technical Safeguard categories simultaneously.
Business Associate Agreements: When Your QR Vendor Becomes a BA
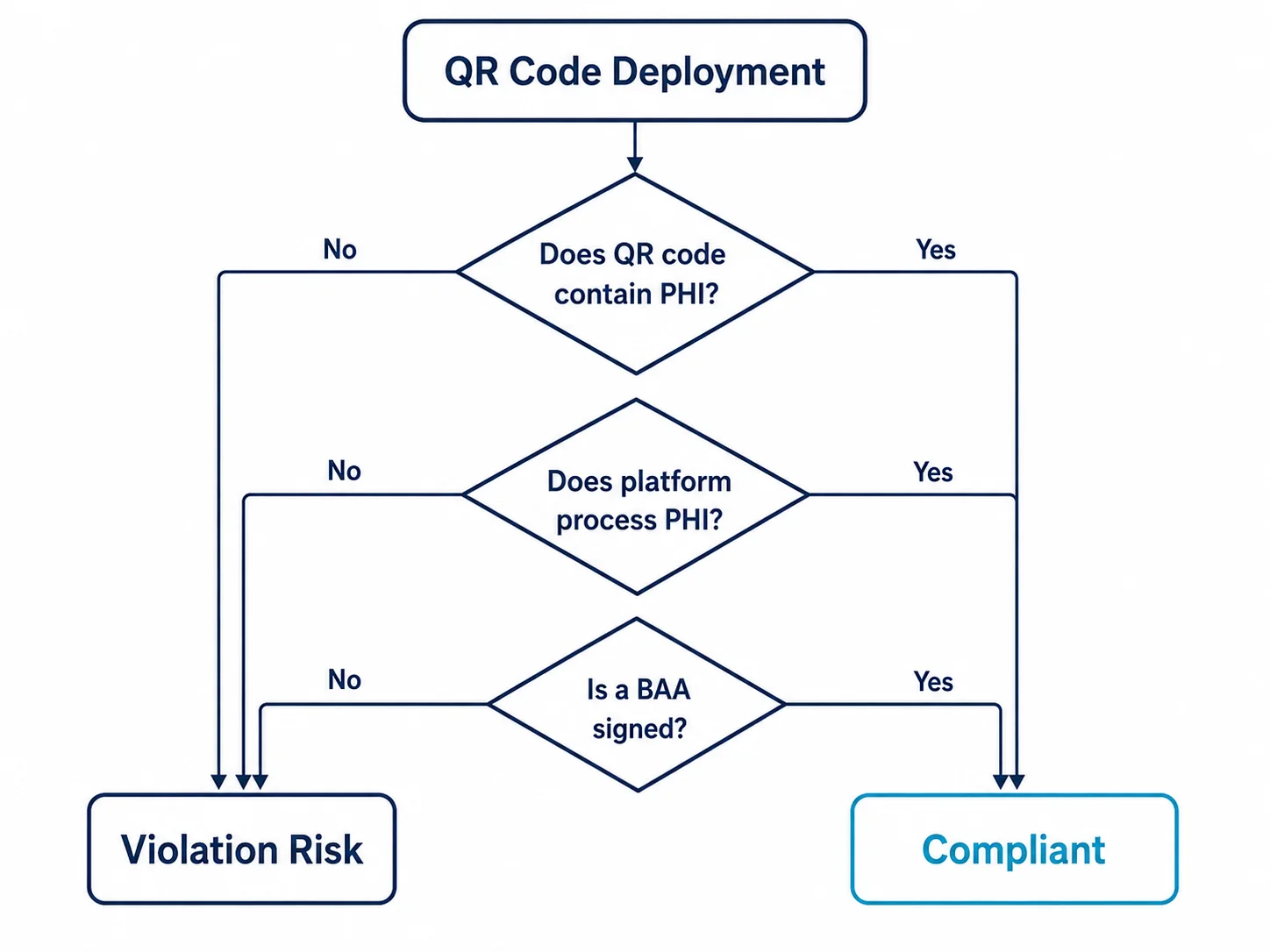
Under 45 CFR § 160.103, a Business Associate is any person or entity that creates, receives, maintains, or transmits PHI on behalf of a covered entity. The key question for QR code platforms: does the platform's infrastructure touch PHI in any form?
For most QR platforms, the answer is yes — even when the platform claims to be "just a redirector." Scan logs that associate a timestamp and a scanner identifier with a specific QR code used in a patient workflow constitute PHI if they can be linked back to an individual patient. HHS guidance from January 2023 confirmed that metadata alone can constitute PHI when combined with contextual information. If your platform logs the IP address of every scan, and you deployed a unique QR code per patient room at check-in, those logs link IP to patient identity.
Before any clinical QR deployment, healthcare IT teams must:
- Conduct a HIPAA risk analysis specifically covering the QR vendor's data flows
- Require the vendor to execute a BAA that explicitly covers scan log data
- Verify the BAA includes breach notification timelines, subcontractor flow-down requirements, and data destruction terms
- Confirm the vendor's incident response SLA — BAA or not, you own the breach notification to patients within 60 days
Vendors who decline to sign a BAA should be disqualified from any PHI-adjacent QR deployment, period. As of May 2026, Flowcode offers a BAA for enterprise healthcare accounts. Bitly's standard terms explicitly exclude healthcare use. Always verify current terms directly with the vendor before contracting.
HIPAA QR Use Cases: What Works and What Gets You Cited
Patient Check-In and Appointment Verification
This is the highest-volume and highest-risk use case. A QR code texted or emailed to a patient before their appointment can replace the front-desk sign-in sheet — but only if the token-based pattern described above is implemented. The 2024 OCR settlement with a Midwest health system ($780,000 in penalties) included a finding that pre-appointment QR codes linked directly to pre-filled patient forms without authentication, exposing PHI to anyone who forwarded the appointment SMS to another device.

Medication Tracking and Administration
QR codes on medication packaging and patient wristbands are low-PHI-risk when used for bedside scanning workflows. The code identifies the medication SKU or administration record ID, not the patient directly. The ePHI linkage happens in the eMAR system that the nurse's scanner connects to, not in the QR code itself. This is one of the cleanest QR use cases from a HIPAA perspective, provided the eMAR system satisfies audit control requirements for every scan event.
Asset and Equipment Tracking
Encoding equipment serial numbers and location data in static QR codes is HIPAA-neutral — no PHI involved. This is a safe starting point for healthcare organizations testing QR infrastructure before moving to patient-facing workflows. Hospitals using this approach report 40–60% reduction in equipment search time according to a 2024 HIMSS survey of 312 health systems.
Patient Education and Discharge Instructions
QR codes on discharge paperwork that link to generic educational content (medication instructions, wound care videos) are generally low-risk if the content is not patient-specific. The risk escalates when the QR code links to a personalized care plan that includes diagnosis, medications, or follow-up instructions. In that case, token-based authentication is required.
When QR Codes in Healthcare Are the Wrong Tool
There are scenarios where QR codes introduce more risk than they solve, and competent healthcare IT teams recognize these limits.
Emergency department triage is a bad fit for QR-initiated workflows. Patients who arrive by ambulance, unconscious, or in acute distress cannot authenticate. Any QR workflow that requires the patient to act is unusable for the highest-acuity cases, which are also the cases where data accuracy is most critical. A manual or wristband-barcode process remains more reliable for ED intake.
Cross-facility deployments with multiple EHR systems create integration complexity that QR codes cannot solve on their own. A QR code resolving to an Epic patient portal cannot authenticate a patient enrolled only in Cerner — the token validation must happen against a single identity system. Multi-vendor environments need a federated identity layer before QR check-in can work across sites.
The Link Shortener Problem: Why Most Generic QR Platforms Fail HIPAA
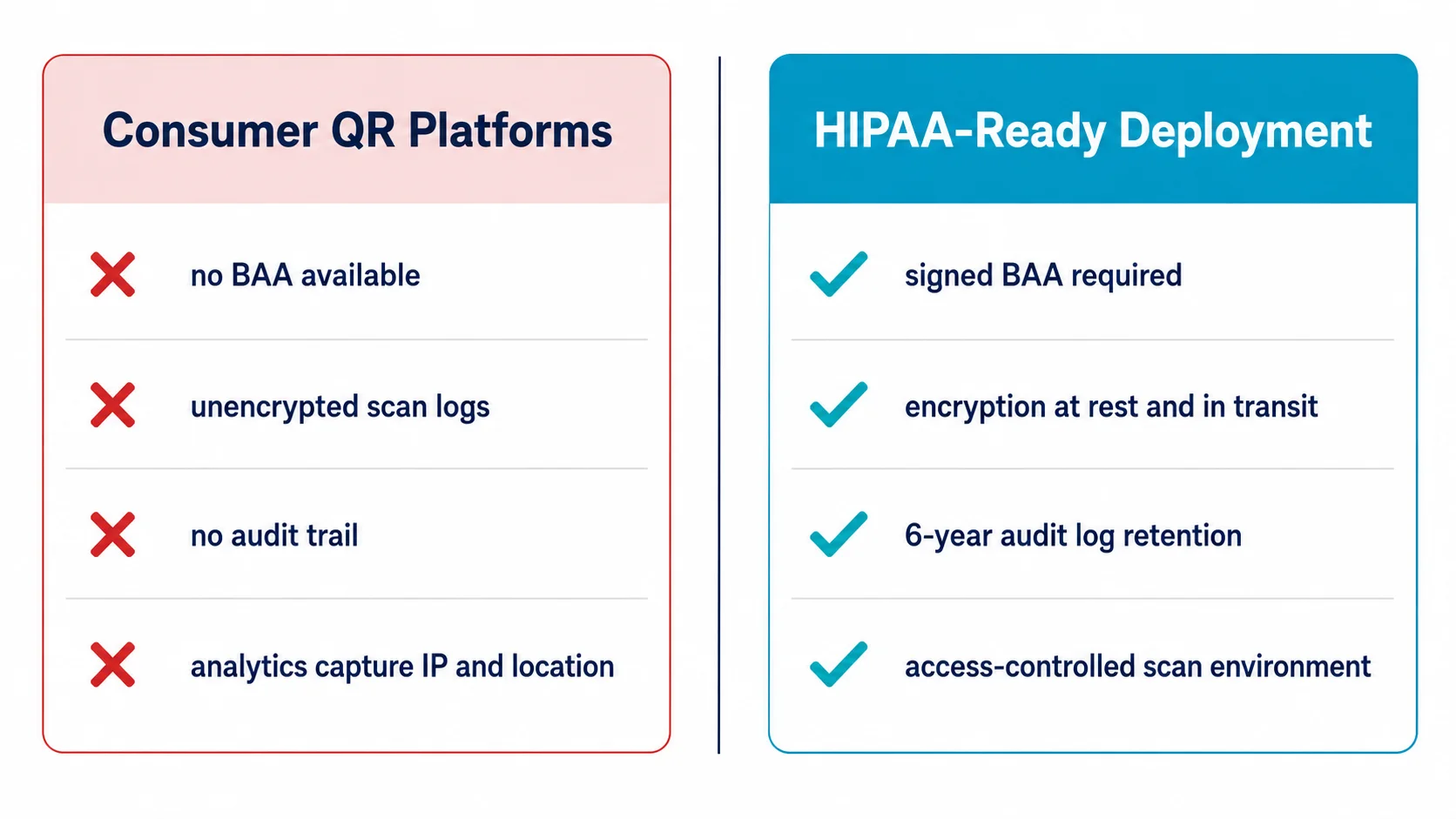
Generic QR code generators — including many marketed to small businesses — use shared link shortener infrastructure for their dynamic redirect functionality. This creates three specific HIPAA failure modes that healthcare IT teams consistently underestimate.
First, shared redirect domains mean your healthcare QR codes resolve through infrastructure also used by e-commerce, marketing, and untrusted third parties. A BAA covering your account on a shared platform cannot extend to the vendor's other customers or their data handling practices. Shared infrastructure is incompatible with HIPAA's minimum necessary principle.
Second, link shorteners typically log full referrer headers. If a patient scans a QR code from within an EHR-generated email, the referrer may contain patient-identifiable URL parameters. The shortener logs these. The shortener vendor now holds PHI without a BAA — an immediate breach.
Third, link analytics dashboards provided by generic platforms often show scan data to all account administrators, not just the healthcare team that deployed the code. HIPAA's access control requirements prohibit PHI exposure to personnel who don't have a legitimate healthcare purpose. Shared analytics dashboards violate this rule by design.
Healthcare deployments require a QR platform with dedicated redirect infrastructure, per-account data isolation, and explicit HIPAA contractual commitments — not a shared-link-shortener backend dressed up with a healthcare landing page.
How QR Nova Approaches Healthcare Compliance
QR Nova's architecture separates static QR code generation — where no server infrastructure is involved post-creation — from dynamic QR redirect management. For healthcare use cases, this distinction matters.
For static QR codes pointing to public-facing content (generic educational materials, department wayfinding, equipment asset tags), QR Nova generates codes that contain only the final URL. No redirect infrastructure, no scan logs, no server touch points. These codes are HIPAA-neutral by design — there is no system in the middle that could create a PHI linkage.
For dynamic QR codes in healthcare environments, the audit trail and access control features provide the logging infrastructure required by § 164.312(b). Every scan event captures timestamp, user agent, and anonymized IP. Destination URL updates require authenticated access with role-based permissions — no anonymous URL modification. Healthcare teams evaluating QR Nova for PHI-adjacent workflows should contact the team directly to discuss BAA execution and deployment architecture review before go-live.
The broader point: any QR platform claiming HIPAA compliance without being willing to discuss their specific data architecture and BAA terms is a vendor to avoid. HIPAA compliance is not a checkbox. It is a continuous operational posture that requires transparency from every vendor in your workflow chain.
Healthcare IT Vendor Checklist: 7 Questions Before You Deploy
Before signing any QR code platform contract for a healthcare deployment, get written answers to these questions:
- Will you sign a Business Associate Agreement? If the vendor hedges, says it's "not necessary," or says their legal team will review for more than 5 business days, treat this as a red flag. BA status is determined by data flow, not by vendor preference.
- Is your redirect infrastructure dedicated or shared? Shared infrastructure cannot satisfy HIPAA's access control requirements for PHI-adjacent workflows. Require a written architecture description.
- What does an audit log entry include? Minimum: timestamp, scanner IP, user agent, destination URL. Ideal: authenticated user identifier when authentication is part of the workflow.
- How long are scan logs retained, and how are they protected? HIPAA requires audit controls — retention policies and access controls on log data itself must be specified.
- Can destination URLs be locked to prevent unauthorized modification? Role-based access control on URL editing is required. A QR code whose destination can be changed by any account user is an integrity control failure.
- What is your breach notification timeline? The BAA must specify notification to the covered entity within a defined window — typically 72 hours for known breaches, to allow the covered entity to meet HIPAA's 60-day patient notification requirement.
- Do you have SOC 2 Type 2 or equivalent third-party attestation? Self-certification is not enough. Third-party audit reports covering availability, confidentiality, and security controls provide the evidence base for your own risk analysis documentation.
Save this list. OCR's Phase 2 audit protocol — the framework used for desk and on-site audits — specifically reviews vendor management documentation. Covered entities that cannot produce BAAs and due diligence records for every vendor in a PHI workflow face significantly higher penalty exposure. For a broader set of deployment standards that apply before and after go-live, review our QR code best practices guide covering print specifications, error correction, and tracking setup.
The 2026 HIPAA Enforcement Environment: Why This Matters Now
OCR's 2025 enforcement statistics show a 34% increase in settlements involving electronic health workflows compared to 2023, with an average settlement value of $412,000. The agency's 2026 enforcement priorities, published in the Federal Register in December 2025, explicitly list "emerging technology deployment without prior risk analysis" as a targeted audit category — and QR code deployments in patient-facing contexts appear in the agency's example case list.
The 2026 HIPAA Security Rule updates, finalized in January 2026 and effective by late 2026, strengthen requirements around encryption (moving from addressable to required for ePHI in motion) and risk analysis frequency (now required annually rather than periodically). Dynamic QR code platforms used in healthcare must meet the new encryption requirements: TLS 1.2 minimum, TLS 1.3 recommended for all new deployments.
Healthcare organizations that deployed QR codes before 2024 without conducting a formal risk analysis covering the QR vendor specifically should treat this as an open audit finding. A documented risk analysis — even one that concludes the risk is acceptable with stated controls — provides substantially stronger enforcement protection than no documentation at all.
The QR code is not the compliance problem. The gap is between what the QR code promises and what the underlying data infrastructure actually does — often: log, store, and transmit patient-linkable data without controls. That gap is where the compliance failures live. QR code HIPAA compliance in healthcare is an architecture and vendor management discipline. Close the gap with the right technical controls, the right vendor contracts, and an annual risk review that covers every system a QR code touches. Then document all of it.
Start with a compliant QR code infrastructure at QR Nova's free QR code generator — no subscription required for static codes, full audit trail available for dynamic deployments.
Frequently asked questions
Are QR codes HIPAA compliant?
A QR code itself is not inherently HIPAA compliant or non-compliant — it's just a link. Compliance depends entirely on what the code points to and how the destination handles protected health information. If the destination collects, stores, or transmits PHI without proper safeguards, you have a HIPAA violation regardless of the QR technology used.
What is a Business Associate Agreement and do I need one for QR codes?
A BAA is a written contract between a covered entity (hospital, clinic) and any vendor who handles PHI on its behalf. If your QR code platform stores scan logs that could contain PHI — like patient identifiers linked to a scan event — that vendor qualifies as a Business Associate and must sign a BAA before you go live. Failure to execute a BAA is itself a HIPAA violation subject to civil penalties.
Can I put patient information directly in a QR code?
No. Encoding PHI directly into a QR code symbol is never HIPAA-compliant. The data is readable by any QR scanner, is not encrypted in transit, and cannot be revoked. The compliant pattern is to encode a short-lived token or authenticated URL that resolves to PHI only after the user is verified.
What HIPAA rules apply specifically to QR codes in healthcare?
The HIPAA Security Rule's Technical Safeguards (45 CFR § 164.312) are the most directly applicable. They require access controls (unique user IDs, emergency access), audit controls (hardware, software, and procedural mechanisms to record access to ePHI), integrity controls, and transmission security (encryption). Every QR-driven workflow that touches ePHI must satisfy all four categories.
What happens if a QR code causes a HIPAA breach?
The covered entity bears primary liability. OCR's enforcement actions from 2024–2025 show penalties ranging from $25,000 for a single corrective action plan to $1.9 million for systemic failures. If a QR platform vendor is implicated and lacked a BAA, penalties can stack on both the covered entity and the BA. The covered entity must also notify affected individuals within 60 days of discovering the breach.
Do static QR codes pose higher HIPAA risk than dynamic ones?
Yes, for PHI-adjacent use cases. A static QR code cannot be rotated, revoked, or access-controlled after printing. If it encodes a URL containing PHI or leads to an unsecured page, the exposure is permanent. Dynamic QR codes allow destination updates, token rotation, and access revocation — essential controls for any clinical deployment.
What should I look for in a HIPAA-compliant QR code vendor?
Seven things: (1) willingness to sign a BAA, (2) TLS/HTTPS enforcement on all redirects, (3) immutable audit logs capturing scanner IP, timestamp, and user agent, (4) access control — ability to restrict who can edit destination URLs, (5) short-lived or one-time-use token support, (6) data processing addendum with explicit PHI handling limits, and (7) SOC 2 Type 2 attestation or equivalent.
Related articles
QR Code Accessibility: WCAG 2.2 & ADA Guide (2026)
QR code accessibility WCAG 2.2 & ADA: alt text, contrast ratios, alternative paths, and screen reader fixes. Practical guide for developers.
QR Code Security Best Practices for Platforms
QR code security best practices for platforms: URL validation, redirect auditing, scan anomaly monitoring, abuse prevention, and enterprise audit logs.
QR Code HIPAA Compliance: Complete Healthcare Guide
QR code HIPAA compliance in healthcare: when QR codes handle PHI, BAA requirements, which platforms comply, and a practical checklist for covered entities.
Create a HIPAA-safe QR code — free
Get started